



Endovascular Graft in Aortic Aneurysm
Endovascular graft application is a non-surgical method that can be an alternative to the conventional surgery in selected cases of aortic aneurysm treatment. The patient stays one night in the intensive care unit and discharges within 3 days.
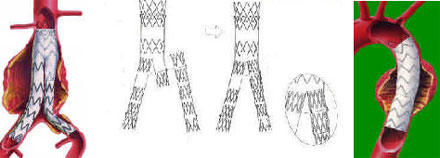
In this operation, leg veins from each pubic are opened as 4-5 cm under the general or local-epidural anesthesia and the graft is sent and inserted into the aneurysm under the radiologic control.
We treated our 117 patients with abdominal aneurysm and 56 patients with thoracic aneurysm with endovascular graft implantation method that is introduced in our country a short time ago. Of the thoracic aneurysms, three were acute dissection (laceration). Return to the conventional surgical method was needed only in three patients. We did not lose any patient during or after the operations. We performed epidural anesthesia in a part of our patients.
THE TEAM:
Chairman of Radiology Department: Prof. Dr. Füruzan NUMAN
Assoc Dr. Harun ARBATLI, Op. Dr. Naci YAGAN, Op.Dr. Oğuz YILMAZ, Op.Dr.Hasan ARDAL
Prof. Dr. Bingür SÖNMEZ
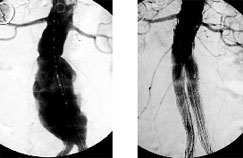
Angiographic view of our first patient before and after the stent.

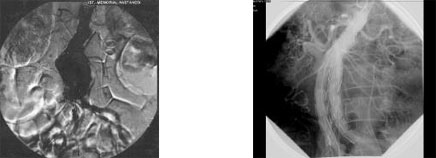
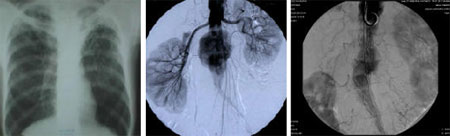
Angiographic view of our second patient before, during and after the operation.

A souvenir photo taken 20 minutes after the endovascular graft operation of our second patient.
Üçüncü hastamız: Kronik lösemi tedavi gören hastamıza önce koroner bypas ameliyatı yapıldı. 2 ay sonra sonra abdominal aort anevrizmasına endostent uygulanan hasta mesane kanseri ameliyatı olmak için beklemektedir.
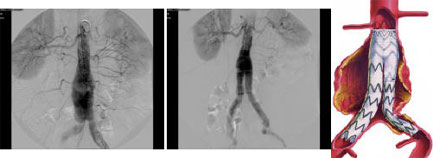
Angiographic view of our forth patient after the endostent operation to the abdominal aneurysm.

Our fifth patient had ischemic heart disease, hypertension, chronic kidney disease (dialysis dependent) and an abdominal aortic aneurysm. To the patient who was impossible to receive general anesthesia, after the complete closure of the narrowing in the right iliac artery under epidural anesthesia, unilateral (aorto unilateral-left) endovascular stent was applied, and then femorofemoral bypass was performed.
Our sixth patient had severe pulmonary tuberculosis and was receiving treatment. Abdominal aortic aneurysm of the patient was 8 cm diameter and needed to be urgently operated. To the patient who was impossible to receive generaş anesthesia, since the right iliac vein was completely blocked, unilateral (aorto unilateral- left) endostent was performed. Femorofemoral bypass was not necessary.